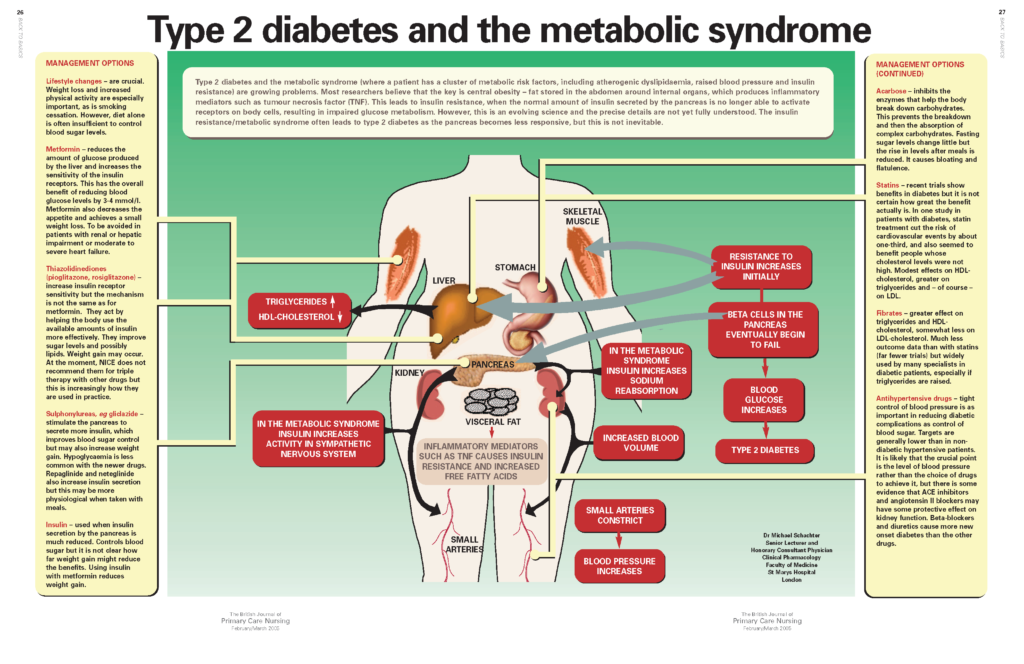
Type 2 diabetes and the metabolic syndrome (where a patient has a cluster of metabolic risk factors, including atherogenic dyslipidaemia, raised blood pressure and insulin resistance) are growing problems. Most researchers believe that the key is central obesity – fat stored in the abdomen around internal organs, which produces inflammatory mediators such as tumour necrosis factor (TNF). This leads to insulin resistance, when the normal amount of insulin secreted by the pancreas is no longer able to activate receptors on body cells, resulting in impaired glucose metabolism. However, this is an evolving science and the precise details are not yet fully understood. The insulin resistance/metabolic syndrome often leads to type 2 diabetes as the pancreas becomes less responsive, but this is not inevitable.
Aspirin in patients with diabetes
Patients with diabetes are at high risk of cardiovascular disease and aspirin is an important part of prevention strategies. Although it is effective and relatively well-tolerated, studies have shown that many patients with diabetes are not taking aspirin. In this article, we review why aspirin should be considered in patients with diabetes, the benefits it might achieve and areas where caution is required.
Making sense of the Quality and Outcome Framework of the new GP Contract
The Quality and Outcome Framework (QOF) of the new GP Contract will be the biggest experiment in improving the quality of care for patients anywhere in the world. By April 2005, we will see how well Primary Care can deliver. In this series, we provide a step-by-step guide on how your practice can get QOF points, including practical information on what data to collect and how to record it. Over the coming months, we will be discussing the best ways to maximise the quality of care and will concentrate on the cardiovascular and diabetes elements of the QOF. We will discuss the setting up of registers, practical tips, examples from practices that are delivering well, how to check how well you are doing from your own IT system and from Quality Management Analysis System and, of course, how to deal with exception reporting and the PCT QOF visit.
Oily fish and cardiovascular disease
The management of cardiovascular disease (CVD) in primary care has been transformed in recent years, particularly with extensive use of statins in secondary prevention. But what about the less high-tech approach of getting patients to eat more healthily? Dietary advice has traditionally been offered primarily to those needing to lose weight or lower their lipid levels. But more recently, systematic reviews have shown good evidence that dietary changes can reduce mortality and morbidity in addition to modifying some risk factors in patients with coronary heart disease. Evidence to date suggests similar benefits of healthier eating are likely in primary prevention. In this new series – Food for Thought – we sort the wheat from the chaff when it comes to dietary advice for patients with cardiovascular disease. This article will focus on the benefits of oily fish, with the good news that simply increasing oily fish intake achieves major benefits.
Practical approaches to empowering people with cardiovascular disease or diabetes
For people with long-term conditions, self-care can have as much, if not more, influence on their health than prescribed medication and treatment. Yet, in many cases, healthcare professionals become frustrated when attempts to improve peoples’ self-care behaviours prove unsuccessful. This article looks at some of the reasons why it can be difficult to encourage people with diabetes or cardiovascular disease to look after themselves effectively; what types of practice can help us to increase people’s success in managing long-term conditions; and how we can incorporate empowering techniques in our day-to-day consultations.
Sex after an MI
Rehabilitation after a myocardial infarction (MI) includes all aspects of a patient’s life – medical, physical and social. Sexual functioning is an important part of most people’s lives. Fears about whether having sexual intercourse could trigger another heart attack is the question many post-MI patients want to ask but embarrassment may stop them. Giving accurate information about sex after an MI is just as much a part of patient education as telling them about cholesterol and blood pressure and can go a long way to helping recovery and preventing further problems such as sexual dysfunction.
Stroke and TIA
Stroke is common, affecting around one in four people over the age of 45 at some time in their lives. Increasing age is a major risk factor for stroke, so the numbers of people suffering a stroke will increase with the ageing population. Primary care teams have a central role in providing effective secondary prevention, but because patients often fall between primary and secondary care, things may be missed. Taking a systematic approach to assessing risk factors, such as blood pressure, and treating them effectively can significantly reduce further stroke risk.
Ezetimibe: a new type of lipid-lowering therapy
Only half of patients being treated for elevated cholesterol levels are currently reaching targets, according to recent research. So what can we do to improve things? One option is to add a new type of lipid-lowering drug – ezetimibe – to a statin. This article reviews how ezetimibe works and its place in primary care management of raised lipids.
Raising the issue of obesity with patients who need to lose weight
You know the scenario only too well. Your patient is sat in front of you, taking up more space than he or she used to, and you are discussing the increase in their blood glucose levels. How do you raise the issue of their weight, without offending them or making what seems to them a personal comment?
Optimising treatment of type 2 diabetes with metformin
There is good evidence that tight glycaemic control significantly improves outcomes in patients with type 2 diabetes. All practice nurses will be looking to achieve the new General Medical Services contract (GMS2) targets for HbA1c reduction in diabetes (see box). Practices will be developing prescribing strategies to achieve this reduction, in accordance with good clinical practice. Metformin offers an important first-line therapy for type 2 diabetes. The introduction of a new, sustained-release formulation – Glucophage SR – should improve patient compliance with metformin and so improve glycaemic control.
Talking to Practices
Rosemary Evans, practice nurse at a Docklands practice, London, talks to BJPCN about why and how she set up her smoking cessation service
Disease Focus on… Angina
Angina is a common problem in primary care, affecting around one in every six patients aged 65 years and over. It ispredominantly chest pain due to transient myocardial ischaemia caused by coronary artery disease. Episodes of angina are typically caused by exertion or emotion, and are relieved by rest. Treatment with drugs and/or surgery that improves blood flow to the heart and lifestyle changes can significantly improve patients’ quality of life and survival.














