There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
Making Best Practice, Every Day Practice

This resource is fully searchable using the search box at the top of the page, or to narrow down your selection using filters click on 'Knowledge hub' in the main navigation.

There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
This case describes a 56-year old male with a productive cough and worsening breathlessness who presented to a practice nurse. This case study was part of a Health Assessment module at the University of Surrey. The case study was supervised by a GP.
People with COPD should be reviewed at least annually according to the Quality and Outcomes Framework. However, there is little mention of the importance of assessing nutritional status and no ‘QOF’ points for doing so. This article describes the assessment and management of COPD patients with a risk of malnutrition.
Chronic Obstructive Pulmonary Disease (COPD) has a major impact on the health and quality of life of patients and there is often co-morbidity with cardiovascular disease. Well planned and structured training for the primary care team could have a major impact on outcomes.
Morbidity and mortality for women with COPD is increasing. This systematic review uncovers how women seem to experience COPD differently to men, and helps health care professionals to provide an individualised approach to caring for these patients.
Heart failure is characterised by fatigue, breathlessness and retention of fluid. The update of the National Institute for Health and Clinical Excellence chronic heart failure guidelines has simplified its management by using a stepped approach to investigation and treatment. In this article, we focus on the practical aspects of managing the two main symptoms associated with heart failure – oedema and breathlessness.
Chronic obstructive pulmonary disease (COPD) is a largely preventable, slowly progressive, inflammatory disease. Rates of COPD are rising faster in women than in men, yet women are less likely to be diagnosed. There is currently no cure, but best-practice management outlined in recently updated NICE guidelines can help to improve patients’ symptoms and quality of life.
Chronic clinical conditions have traditionally been regarded as individual disease categories within individual patients, although there is often considerable overlap across clinical systems. However, for those managing these patients the presence of various co-morbidities is all-too apparent. It may be time to consider a new approach to management of these patients.
Cardiovascular morbidity and mortality in patients with chronic obstructive pulmonary disease (COPD) is nearly double the rate in the general population without COPD. And for those with cardiovascular disease (CVD) and COPD, heart failure is the most common cause of hospitalisation.
Chronic clinical conditions have traditionally been regarded as individual disease categories within individual patients, although there is often considerable overlap across clinical systems. The monitoring of patients with long-term conditions has historically centred around a traditional model of a nurse-led clinic, utilising an appropriate level of skill mix. The disease categories and associated clinical indicators of the Quality and Outcomes Framework (QOF) have encouraged this approach, but for those managing these patients the presence of various co-morbidities is all too apparent
Chronic obstructive pulmonary disease (COPD) is the term used to describe a range of
chronic chest conditions, including chronic bronchitis and emphysema. COPD is
characterised by permanent damage to the lungs and as the condition develops, people
experience increasing breathlessness, to the point where even everyday activities such
as getting dressed or walking up stairs become difficult. This article describes the impact of
COPD, explores the value of exercise in COPD management and discusses possible reasons for its
widespread under-use as effective symptom control.
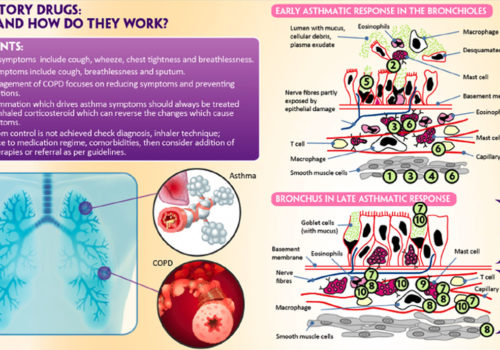
One person in every five households in the UK is receiving treatment for asthma,
according to latest figures. As well as treatment for asthma, many of these individuals
also self-medicate for minor illnesses or require prescribed medication for other
conditions. It is important that the drugs they take do not adversely affect their asthma
control. In this article we review which drugs might cause problems in patients also taking
treatment for asthma.
The BJPCN interviewed Dr Steve Holmes (Chairman of the GPIAG) and
Stephanie Wolf (GPIAG General Committee member) on the 20th anniversary
of the organisation.














A unique new e-platform for primary care

By continuing to this site you are confirming that you are a healthcare professional and are opting into the use of cookies.