There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
Making Best Practice, Every Day Practice


About asthma and allergies
Asthma and allergies result in multiple long term consultations with an estimated 1 in 12 adults and 1 in 11 children in the UK. Sadly death rates remain stubbornly high will an average of three deaths a day.
Currently asthma costs the NHS about £1 billion p.a. and results in about 80,000 hospital admissions.
Allergy is affecting an increasing number of British adults and today they affect up to 44% of the population. Most allergies are not life threatening but in severe cases they cause anaphylaxis which may be fatal.
These resources include:
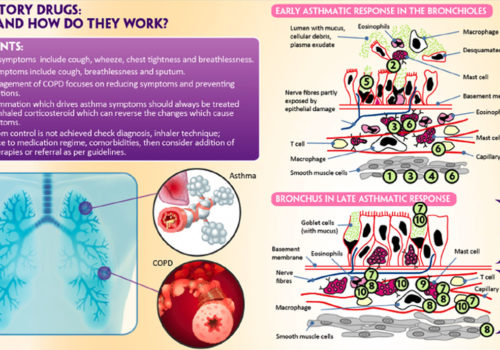
![]() Explanations of the etiology of asthma and triggers of acute asthma attacks
Explanations of the etiology of asthma and triggers of acute asthma attacks
![]() The spectrum of asthma medications including inhaled corticosteroids, long-acting beta agonists (LABAs), leukotriene modifiers and inhalers combining a corticosteroid and a LABA
The spectrum of asthma medications including inhaled corticosteroids, long-acting beta agonists (LABAs), leukotriene modifiers and inhalers combining a corticosteroid and a LABA
![]() Reviews of recent asthma management guidelines and their application in primary care
Reviews of recent asthma management guidelines and their application in primary care

![]() Techniques and guidance to improve inhaler technique in children and adults
Techniques and guidance to improve inhaler technique in children and adults
![]() Articles also discuss common allergies such as allergic rhinitis and urticaria and the safe use of antihistamines
Articles also discuss common allergies such as allergic rhinitis and urticaria and the safe use of antihistamines
There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
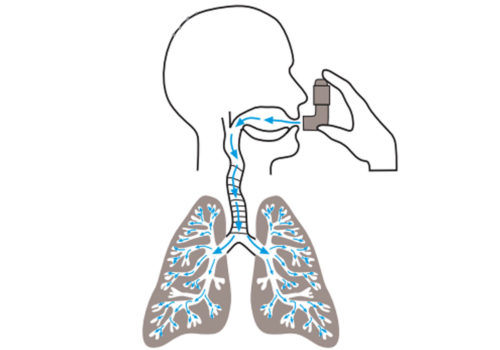
Asthma UK estimates that 2.1 million patients in the UK are suffering unnecessarily because
they do not use their asthma treatment effectively. This article looks at how inhaled
therapies are deposited in the lungs, and at the basic differences between inhalers – with
a focus on optimising inhaler technique.
The current treatment of asthma in the UK is rightfully seen as a triumph of chronic disease management within a primary care setting. Almost all routine asthma care and, increasingly, elements of acute asthma care, are now provided in general practice. Over the past twenty years, significant effort and investment have gone into the production […]
One person in every five households in the UK is receiving treatment for asthma,
according to latest figures. As well as treatment for asthma, many of these individuals
also self-medicate for minor illnesses or require prescribed medication for other
conditions. It is important that the drugs they take do not adversely affect their asthma
control. In this article we review which drugs might cause problems in patients also taking
treatment for asthma.
Asthma is a chronic disease that has, for a long time, been the domain of primary care nurses, and many have qualifications enabling them to run nurse-led asthma clinics. It is, therefore, essential to fully understand the Quality and Outcomes Framework (QOF) and to be able to maximise the points available to the practice, at the same time as providing a comprehensive service to patients. In this article, we review the QOF indicators for asthma, strategies for optimising record keeping and performing asthma reviews.
More than half of people with asthma in the UK have inadequate symptom control,
despite the range of effective therapies now available. Rather than blaming
patients when they fail to take their medications as prescribed, we need to
examine the way we conduct asthma consultations and ask whether we are failing
to meet the needs of individual patients. How can we gain greater understanding about what
people with asthma want from healthcare professionals and treatments, so we can achieve a
more patient-centred approach to care?
On 23 June 2005, the Met Office issued a warning that severe thunderstorms were likely
to hit the South East of England in the next 24 hours. On the evening of Friday 24 June,
primary care out-of-hours services and hospital accident and emergency departments
in Northwest London were inundated by patients attending with acute asthma. The
scale of these attendances – eight times more patients than usual in one hospital – meant that
departments had to call in additional staff and some ran out of emergency supplies of
bronchodilators, nebulisers and oral steroids for treating asthma. In this article, we will explain
the background and some of the theories related to this type of epidemic of acute asthma –
Thunderstorm Asthma.
Beta agonists are the only class of drugs that is recommended for the management of
asthma at every level of current guidelines, including those from the British Thoracic
Society (BTS). This means that they are used across the spectrum of severity of
asthma, from mild intermittent disease (step one) to severe asthma symptoms (step
five). In this article, we take you through the key things that you – and your patients – need to
know about these drugs.
We continue our series on the changing role of the community pharmacist, with an article
from Alpana Mair in Edinburgh describing the work of a pharmacist in COPD and asthma
clinics based on her experience.
The Quality and Outcomes Framework (QOF) is now well into its third year and continues
to expand boundaries of quality domains within chronic disease management. In this
article we review some of the challenges in QOF indicators for asthma and COPD and
suggest some tips to make the requirements easier to achieve in daily clinical practice.
Breathlessness is a very common problem in the patients we see in general practice, and
there is a range of possible causes. In this article – the first in a series of three looking
at how to diagnose what’s wrong with a breathless patient – we explore how to
distinguish between two of the commonest respiratory causes of breathlessness,
asthma and chronic obstructive pulmonary disease.
Good self-management is obviously a central part of achieving effective control of any
chronic condition. It is particularly important in asthma to help patients manage
exacerbations, which can sometimes develop with little warning and with serious
consequences. This article provides a step-by-step guide to developing effective selfmanagement
plans for patients with asthma by providing practical solutions to key questions
underpinning the process.














A unique new e-platform for primary care

By continuing to this site you are confirming that you are a healthcare professional and are opting into the use of cookies.