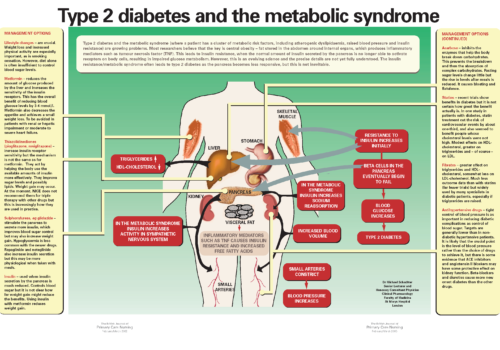
Type 2 diabetes and the metabolic syndrome (where a patient has a cluster of metabolic risk factors, including atherogenic dyslipidaemia, raised blood pressure and insulin resistance) are growing problems. Most researchers believe that the key is central obesity – fat stored in the abdomen around internal organs, which produces inflammatory mediators such as tumour necrosis factor (TNF). This leads to insulin resistance, when the normal amount of insulin secreted by the pancreas is no longer able to activate receptors on body cells, resulting in impaired glucose metabolism. However, this is an evolving science and the precise details are not yet fully understood. The insulin resistance/metabolic syndrome often leads to type 2 diabetes as the pancreas becomes less responsive, but this is not inevitable.